How Much Protein Do We Actually Need?

This piece is the first in a series called Polemics on Protein, which addresses several topics surrounding the consumption of protein.
As always, any cited scientific research that is open source will be bolded and italicized.
Vegans the world over are consistently asked one question: "so, how do you get your protein?"
One quickly learns to prepare a stock response, listing protein powder, oats, peanut butter, legumes, quinoa, and pasta.
In the same breath, I now retort, "how much protein do we actually need to consume on a daily basis?"
Odds are the interlocutor will not know, just as most Americans are likely unaware of the putative protein requirements handed down by the U.S. government. The Food and Drug Administration (FDA) currently places this value at 50 grams/day.
Another governmental agency, the Food and Nutrition Board, more precisely places the recommended daily allowance (RDA) for protein at 0.8 grams per kilogram (kg) of body weight for both male and female adults. When converted for American sensibilities, this comes to 0.36 grams of protein per pound of body weight.
This recommendation has in fact changed little since 1941, when 1 gram of protein per kilogram of bodyweight was recommended for men and about 1.07 grams per kg for women.
As the average American male weighs 200 pounds and his female counterpart weighs 170 lbs., the RDA for protein comes to 72 grams and 61 grams, respectively.
Emerging research, however, shows that this recommended amount is likely to be severely inaccurate and following this guideline could be detrimental.
Optimal Protein Intake
The protein RDA is not necessarily an appropriate guideline to follow when considering the “optimal” protein (nitrogen) intake to promote morphological, physiological, and health-related changes in skeletal muscle, a component of lean mass.
Historic guidelines for protein requirements were based on nitrogen balance studies. The amount of nitrogen intake through protein consumption is compared to the amount of nitrogen excretion, mainly in the urine and feces.
When intake is higher than excretion, there is a “positive nitrogen balance,” in which synthesis of proteins in the body (including skeletal and smooth muscle protein as well as the proteins that make up enzymes, hormones, hemoglobin, and antibodies) occurs to a greater degree compared to protein breakdown and turnover.
Conversely, when intake is lower than excretion, there is a “negative nitrogen balance,” and protein breakdown outpaces protein synthesis.
When intake is roughly equal to excretion, protein synthesis is assumed to occur at a similar rate to protein breakdown. This amount of dietary protein is therefore deemed the body’s basic “requirement” for daily consumption.
This process might sound neat and organized but evaluating nitrogen balance requires a minimum of three days of arduous data collection of all sources of food intake and excrement after which the final calculation of nitrogen balance may still result in wide variability (Pencharz & Ball, 2003; Pencharz et al., 2016). The participants in these studies, moreover, were mostly college-aged men (Wolfe et al., 2008).
Despite these considerable faults, the Food and Nutrition Board (as well as virtually all other agencies) makes its recommendations for protein consumption based solely on nitrogen balance research.
Due to the shortcomings of this approach, in the early 2000s investigators began using a novel technique called indicator amino acid oxidation (IAAO).
In this method, a subject's breath is monitored for amino acid metabolism (in the form of oxidation), which enables a more precise estimate of amino acid requirements and thus overall protein needs. (For interested readers, further explanation of this technique is discussed in the Appendix.)
When directly compared to nitrogen balance studies, IAAO led to calculated protein requirements that were 12 to 50% higher than the stipulated RDA (Humayun et al., 2007), a finding corroborated by further IAAO studies (Elango et al., 2008).
These data suggest the RDA for protein should increase from 0.8g/kg of body weight to about 0.9 to 1.2g/kg of body weight. This guideline holds for healthy sedentary adults and healthy sedentary older men.
Healthy sedentary older women may require protein intake closer to 1 to 1.3 g/kg of body weight.
Bear in mind that this benchmark represents the bare minimum to prevent a net loss of protein in the body during energy balance (when energy intake is roughly equivalent to total energy expenditure). These values likely do not reflect the level of consumption necessary for optimal physiologic and physical functioning.
Additional IAAO studies identify the following guidelines:
Healthy active adults in energy balance (i.e., caloric intake roughly matches total energy expenditure) or energy surplus (i.e., caloric intake exceeds total energy expenditure): 1.6 to 2.2g/kg of body weight (0.73 to 1g/lb. of body weight)
Consumption of protein above 2.2g/kg/day may not increase lean mass accretion or strength during energy balance or surplus
Healthy active adults in energy deficit (i.e., caloric intake is less than total energy expenditure): 1.8 to 2.7g/kg of body weight (0.82 to 1.2g/lb. of body weight)
Older adults who are healthy and active, with an acute or chronic illness, or with a severe/critical illness: 1.2 to 1.5g/kg of body weight
Certain guidelines advocate for greater than 1.5g/kg/day during critical illness
Let's revisit our earlier calculations with these new guidelines in mind:
The average American male weighing 200 lbs. should consume 82 to 110 grams of protein if sedentary and 136 to 200 grams of protein if active.
In an energy deficit, this individual should consume 164 to 240 grams of protein
The average American female weighing 170 lbs. should consume 69 to 96 grams of protein if sedentary and 116 to 170 grams of protein if active
In an energy deficit, this individual should consume 140 to 204 grams of protein
This Protein Intake Calculator integrates findings from many of the evidence-based guidelines cited above.
In A Simpler Approach to Health, I argue that protein consumption should primarily, if not exclusively, stem from plant-based sources. Consuming plants over animals holds tangible benefits to both individual and planetary health without consistently observed decrements in lean mass or strength accretion.
Optimizing protein consumption among older adults can aid in preventing loss of muscle mass, muscular strength, bone density, and immune function, all of which are major contributors to frailty and loss of autonomy in older adults (Genaro et al., 2010; Phillips et al., 2016; Lesourd 2004). Although there is no silver bullet to halt the effects of aging, consuming enough protein is certainly a step in the right direction.
Note that older populations also tend to suffer from anabolic resistance, a reduced ability to absorb dietary protein and diminished muscle protein synthesis due to age-related changes in insulin resistance, mobility, and inflammation (Aragon et al., 2023).
Moreover, there is a natural loss of appetite over the lifespan (deemed the “anorexia of aging”) and increased incidence of gastrointestinal disturbances with age, preventing adequate protein intake and contributing to broader malnutrition.
Taken together, older individuals are perhaps the group most in need of optimal protein consumption and at the highest risk of not being able to meet it.
I discuss specific approaches for older adults to optimize protein consumption in a follow-up post.
Appendix
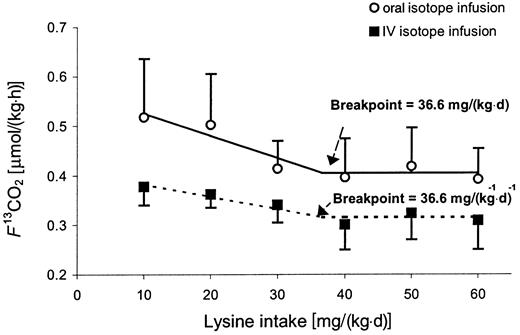
In IAAO, a patient is fed a diet deficient in one essential amino acid. The patient then consumes food items that solely contain this particular amino acid with a carbon isotope label. To be integrated into proteins, the amino acid will be metabolized through a process called oxidation, which will release the isotope label. Based on the amount of isotope detected in the patient's exhaled carbon dioxide, the rate of oxidation can be measured.
As the patient ingests more of this amino acid, the initial deficiency (stemming from their initial diet) will be corrected, leading to a spike in oxidation as previously absent proteins are built anew. As the body approaches its requirement for this amino acid, oxidation decreases and then plateaus at a steady baseline rate. At this baseline "breakpoint" level, at which there are no further changes in oxidation, the patient's requirement for this particular amino acid can be deduced based on the overall amount they consumed (Elango et al., 2008).