

VO2 Max: Unlocking a Key to Longevity

Human physiology exists as an intricate tapestry. Near-constant interplay between our cardiovascular, respiratory, and metabolic systems maintains a precise equilibrium of oxygen, hydrogen ions, and glucose within our blood, ensuring adequate cellular function, energy production, and removal of toxic byproducts.
A metric of cardiorespiratory fitness known as VO2 max sits at the nexus of these dynamic processes. VO2 max refers to the maximum rate (V) of oxygen (O2) one can extract from inhaled air (using the lungs and blood), transport to exercising muscle (using the heart and blood), and utilize through cellular metabolism (using skeletal muscle, namely mitochondria).
VO2 max is typically measured in milliliters (ml) of oxygen per kilogram (kg) of body mass utilized in one minute (min), giving us the somewhat clunky unit, ml/kg/min. Alternatively, VO2 max may be expressed in absolute terms as liters (l) of oxygen utilized per minute (min), l/min.
Beyond these technical definitions, the deeper utility of VO2 max lies as a crucial marker of overall health and function. In our pursuit of a long, healthy life, optimizing our VO2 max emerges as a vital objective.
VO2 Max as a Measure of Function and Health
VO2 max encompasses the concept of "functional capacity,” the ability to perform tasks and activities essential to daily life with relative ease and efficiency. A higher VO2 max equips individuals with the physiological reserves needed to meet the demands of maintaining independence in older age.
Sitting quietly requires a VO2 max of about 3.5 ml/kg/min
Walking at a pace of three miles (5km) per hour, about 12 ml/kg/min
Ascending a single fight of stairs, about 16 to 17.5 ml/kg/min
Walking with groceries (15 lbs, or 6.8 kg), about 17.5 ml/kg/min
Mowing a lawn, about 19 ml/kg/min
Running at a pace of five miles (8.3 km) per hour, about 29 ml/kg/min
A helpful visualization made by Jayson Gifford, PhD helps to put these values into further context:
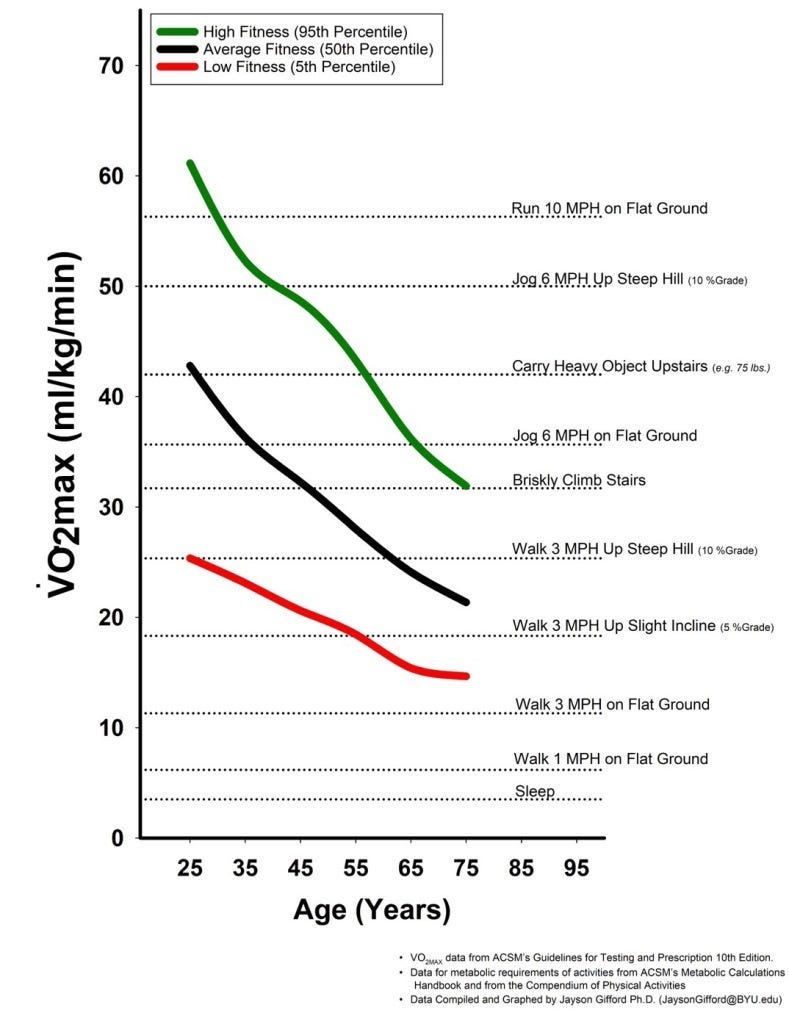
A VO2 max of 50 ml/kg/min corresponds to a male's ability to run a ten-minute mile at a 10% incline. Walking a twenty-minute mile at the same incline equates to a VO2 max of 25 ml/kg/min.
Dr. Gifford separates these data into three groups, suggesting that for males in the 95th percentile of VO2 max at age 75, briskly climbing stairs remains a feasible activity. Such exertion, however, would not be possible for a man in the bottom 5th percentile even at age 25.
Living independently in the eighth decade of life may require a VO2 max around 18 ml/kg/min and 15 ml/kg/min for males and females, respectively.
After reaching the age of thirty, VO2 max decreases by approximately 10% per decade. Among sedentary individuals aged 50 to 75, this decline may escalate to 25% per decade, with males experiencing a more pronounced decrease. This gradual reduction is attributed to the stiffening of both heart muscle and arterial walls in addition to decreases in maximal heart rate, blood volume, and muscle mass.
This decrement is not destiny. Endurance athletes who continue training into older age see a reduction of only 4 to 6% in VO2 max each decade, about 80% lower than their sedentary peers. We will discuss discrete training parameters to attain and maintain high VO2 max later in this piece.
In considering these data, it is important to acknowledge that individuals with disabilities may not possess the capacity to engage in certain activities as a baseline. I do not intend to suggest that an inability to walk a certain distance or ascend stairs is a mark of infirmity or poor health.
Separate from its demarcation of function, VO2 max is likely more predictive of mortality than more traditional risk factors like coronary artery disease, high blood pressure, smoking, and diabetes assessed in isolation. In other words, VO2 max effectively aggregates the impact of these other metrics into a single composite value, making it a mortality risk calculator unto itself.
More importantly, when removing the influence from obesity, smoking, cholesterol levels, family history of heart disease, and diabetes in predicting mortality, VO2 max remains a significant, independent risk factor. Therefore, if we only change VO2 max and hold all other risk factors constant, we can expect to alter mortality risk.
When paired with more conventional risk factors, VO2 max has the ability to increase the accuracy of risk predictions, leading to increasing calls to integrate VO2 max as a clinical vital sign.
Numerous studies detail the significant association between VO2 max and all-cause mortality. Perhaps the most seminal work followed 122,000 patients referred for an exercise stress test over an average of eight years after their VO2 max was measured. Over that time, participants in the lowest quartile of VO2 max (i.e., the bottom 25%) experienced all-cause mortality at a rate 290% higher than those in the top quartile (the top 25%).
Other evidence suggests that each 3.5 ml/kg/min increase in VO2 max may decrease the risk of all-cause mortality by 11% (average follow-up of 35.4 years), heart disease mortality by 15-16% (14.9 year follow-up), and cancer mortality by 13% (12.7 year follow-up).
Certainly, we must exercise caution regarding the potential influence of healthy user bias in interpreting these data. A higher VO2 max may simply reflect a combination of favorable genetic traits, socioeconomic advantages, access to healthcare, and various "healthy" lifestyle choices beyond physical activity, such as maintaining a balanced diet and refraining from smoking or excessive alcohol consumption.
Randomized clinical trials fortunately provide a clear signal. Structured physical activity enables individuals from diverse backgrounds to not only improve their VO2 max but also realize significant reductions in mortality risk and enhance their quality of life.
Among middle-aged patients with chronic heart failure, a 6% increase in VO2 max (0.4 ml/kg/min) over three months was associated with a 5% lower risk of all-cause mortality and all-cause hospitalization after controlling for other risk factors
Among younger and older patients with type two diabetes, a 21% increase in VO2 max (5.3 ml/kg/min) over twelve weeks was associated with a 0.58-point reduction in HbA1c, which roughly corresponds to an 8% reduction in all-cause mortality risk
Among middle-aged sedentary men, a 21% increase in VO2 max (5.6 ml/kg/min) over 24 weeks was associated with a 15% decrease in LDL cholesterol (9.4 mg/dL), which corresponds to 5% lower risk of all-cause mortality
Among older adults with treatment-resistant hypertension, a 7% increase in VO2 max (1.4 ml/kg/min) over 8 to 12 weeks was associated with a five-point reduction in systolic blood pressure, corresponding to a 6.5% lower risk of all-cause mortality
Among middle-aged adults with depression, an 11% increase in VO2 max (2.7 ml/kg/mind) over 16 weeks was associated with a 47% decrease in depressive symptoms
Among pre-pubescent children with obese BMI, a 6% increase in VO2 max (1.9 ml/kg/min) over three months was associated with a seven-point reduction in systolic blood pressure
Why does this association exist?
Consistent exercise training helps to counteract the stiffening of heart muscle and arteries associated with a sedentary lifestyle as we age, enabling the cardiovascular system to accommodate a greater volume of oxygenated blood from the lungs. Exercise further enhances the heart's ability to pump blood throughout the body, particularly to skeletal muscle, which becomes more efficient in producing energy.
These changes manifest as reductions in blood pressure, blood sugar, cholesterol levels, and inflammation, underpinning the protective effect of physical activity on cardiovascular and all-cause mortality.
Who can improve VO2 max?
Further clinical trials consistently demonstrate that structured physical activity can lead to improvements in cardiorespiratory fitness for practically everyone, including younger and older adults who do not currently exercise. (It is again important to recognize that not all individuals can participate in exercise equally due to varying ability levels and environmental barriers.)
In a comprehensive meta-analysis of 41 trials involving a total of 2,100 previously sedentary subjects (average age of 60), engaging in 30- to 35-minute sessions of moderate-intensity exercise three times a week for approximately five months resulted in an average improvement of 16.3% in VO2 max.
Similarly, another meta-analysis comprised of 66 trials and nearly 4,000 participants with overweight or obese BMI (median age of 46) found that structured moderate- or high-intensity exercise led to enhancements in VO2 max by approximately 3.9 to 4.8 ml/kg/min, respectively, over a median duration of twelve weeks.
To summarize these findings:
VO2 max is a useful stand-alone aggregate value for all-cause mortality risk
VO2 max modifies all-cause mortality risk independently of other risk factors
A wide range of individuals— if not virtually all individuals— can meaningfully change their VO2 max
Changes to VO2 max meaningfully modify risk for all-cause mortality and affect important health metrics
How is VO2 Max Measured?
The gold standard for measurement of VO2 max involves subjecting individuals to progressively strenuous exercise on a treadmill or stationary bicycle while monitoring their oxygen consumption, carbon dioxide production, and ventilation. Oxygen consumption increases in tandem with the intensity of exercise increases until a threshold is reached in which additional oxygen cannot be consumed despite further increases in workload. This plateau represents the individual's VO2 max, marking the upper limit of their aerobic capacity.
This form of maximal exercise testing is both expensive and time-consuming and may also be unsafe for patients with pre-existing cardiovascular disease. Less invasive methods of determining one's VO2 max through "submaximal exercise" have gradually been developed:
maximum distance walked or run in twelve minutes (Cooper test);
time to complete a one-mile walk and heart rate at completion;
time to complete a 1.5-mile run or walk;
maximum heart rate (an estimate based on age) and resting heart rate
Free VO2 max calculators can be found at mdapp.co.
On average, data from submaximal exercise testing may differ from an individual’s true VO2 max (as measured through maximal exercise testing) by about 3.5 ml/kg/min on average.
The Apple Watch, one of the most popular smartwatches in the world, began reporting VO2 max estimates in 2020. Apple uses a propriety algorithm that incorporates a user's age, weight, sex, medications that affect heart rate, and heart rate data from walking, running, and hiking workouts on flat ground.
As these VO2 max estimates were validated against submaximal measurements, the reported values on an Apple Watch may on average deviate from an individual's true VO2 max by about 4.9 ml/kg/min. (VO2 max estimates on the Apple Watch may differ from submaximal values by 1.4 ml/kg/min; as noted, submaximal values tend to vary from true VO2 max by 3.5 ml/kg/min. 1.4 plus 3.5 is 4.9.)
Other research indicates that when true VO2 max changes, the Apple Watch estimates also adjust to a comparable degree. Despite potential inaccuracies in the stated values, capturing shifts in cardiorespiratory fitness over time with precision arguably holds greater significance in the long run.
While we should take the reported values on the Apple Watch with a grain of salt and consider utilizing other submaximal estimates modalities to obtain a more accurate VO2 max, the wearable may nonetheless by helpful in monitoring progress over time.
How High Should We Aim?
Provided a consistent exercise regimen is undertaken safely and sustainably, there are virtually no disadvantages to attaining and maintaining a high VO2 max for as long as possible.
The aforementioned seminal work that followed 122,000 participants over an average of eight years stratified VO2 max values into five groups:
Low: VO2 max values in the <25th percentile of the population studied
Below Average: 25th to 49th percentile
Above Average: 50th to 74th percentile
High: 75th to 97.6th percentile
Elite: ≥97.7th percentile
Recall that the group in the highest quartile (High and Elite) was observed to have a 290% lower rate of all-cause mortality during the follow-up period. Attaining a VO2 max within the “High” or “Elite” standards as listed below is therefore a worthwhile goal.


How to Improve Your VO2 Max
Both moderate-intensity and high-intensity cardiovascular exercise are capable of improving VO2 max. In another piece, I delineate moderate-intensity exercise as “Zone 2” and high-intensity exercise as “Zone 5.” Although each zone technically refers to particular blood lactate levels, there are several non-invasive means to approximate intensity:
Talk Test: in Zone 2, you can maintain a conversation without becoming breathless, although it is obvious you are exercising. In Zone 5, you can only say two or three words at a time without pausing for a breath.
Another marker of Zone 2 intensity is the ability to sing the alphabet and reach the letter G without taking an additional breath.
Rate of Perceived Exertion (RPE): a subjective measure of intensity on a scale from 1 to 10, in which 1 is minimal exertion and 10 is maximal exertion. Zone 2 is about 5 to 6 (moderate effort), while Zone 5 is about 8 or 9 (very intense effort but submaximal).
Heart Rate: even though Zone 2 and Zone 5 are distinct from conventional heart rate zones, following your heart rate during a workout will likely prove easier than attempting to hold a conversation with yourself every few minutes. Additionally, RPE can be an especially crude tool and not always intuitive, although some may prefer RPE over monitoring heart rate.
In this Google Sheet, which can be copied to your personal Google Drive, I explore heart rate parameters for Zone 2 and Zone 5 based on age.
On balance, vigorous physical activity is likely more effective at increasing cardiorespiratory fitness. As many as 40% of individuals performing structured moderate-intensity exercise may not experience improvements in VO2 max.
Vigorous exercise frequently takes the form of high-intensity interval training, or HIIT. An exercise is performed at a high-intensity for a particular length of time followed by a rest period of equal or shorter length. This structure is then repeated throughout a session.
Meta-analyses of clinical trials investigating HIIT find that high-intensity intervals lasting 2 to 5 minutes in sessions at least 15 minutes within a training period of 4 to 12 months lead to more significant gains in VO2 max compared to moderate-intensity continuous exercise.
Designing a Zone 5 session is wholly dealer’s choice provided the above specifications are met. For instance, one could perform two five-minute high-intensity intervals with a single five-minute rest period in between for an overall session time of 15 minutes.
In terms of exercise choice, running, cycling, and rowing will likely lend themselves best to high-intensity training. Walking might be feasible, but it will likely be necessary to find a steep hill, use a treadmill at a steep incline, or carry weight in a backpack to reach the intended level of intensity.
A Trip to Norge
Within the literature, the Norwegian 4x4 protocol is among the most researched HIIT structures.

Each workout begins with a 5- to 10-minute warm-up at about 70% of maximum heart rate (MHR).
Following the warm-up, perform four 4-minute intervals of work (hence, 4×4) at 85-95% MHR.
After each interval, actively recover (i.e., keep moving) at about 70% MHR for three minutes before progressing to the next interval.
You might need to briefly stop exercising entirely for your heart rate to decrease to 70% of its maximum during your rest periods. Your heart’s ability to quickly slow down during lower-intensity exercise should improve over time.
At the end of your fourth interval of work, proceed directly into a cool-down for 5 to 10 minutes, aiming to keep your heart rate under 70% of its maximum.
Again, you might find yourself briefly stopping all movement in order for your heart rate to recover adequately.
Not including the warm-up or cool-down, this session should take 25 minutes, as 4×4-minute intervals = 16 minutes and 3×3-minute rest periods = 9 minutes.
Maximum heart rate can be estimated using one of the following formulas:
MHR = 220 - (age)
MHR = 206.3 - (0.711 x age) (Londeree and Moeschberger formula)
MHR = 217 - (0.85 x age) (Miller formula)
Here is a free calculator.
There are several ways to modify the Norwegian 4x4 protocol to decrease its difficulty:
Increase your rest periods to be the same length as your working intervals (each four minutes)
To shorten the overall session, the intervals could be reduced to 3 minutes and rest periods reduced to 2 minutes, or you could do one to two fewer four-minute intervals
Each high-intensity interval should still be at least two minutes and the overall session should not be shorter than 15 minutes in length (exclusive of a warm-up or cool-down)
To extend the session, additional four-minute intervals could be attached.
When performed three times a week, the Norwegian 4x4 protocol led to a 7.2% increase in VO2 max over eight weeks in healthy males and 4.2% in healthy females. Among both male and female participants, performing the 4x4 protocol three times a week contributed to a 10% increase in VO2 max over six weeks and between a 12% to 15.1% increase over eight weeks.
When modified for walking instead of running, 4x4 intervals were also shown to boost VO2 max by 17.9% over ten weeks in male and female subjects with stable coronary artery disease.
Sample Training Block
The Physical Activity Readiness Questionnaire (PAR-Q) helps to determine who should seek advice from a healthcare provider before embarking on a new exercise regimen. If answering yes to any of these questions, consulting with a provider is best practice to understand specific limitations or modifications that may be required.
Has your doctor ever said that you have a heart condition and that you should only do physical activity recommended by a doctor?
Do you feel pain in your chest when you do physical activity?
In the past month, have you had chest pain when you were not doing physical activity?
Do you lose your balance because of dizziness or do you ever lose consciousness?
Do you have a bone or joint problem that could be made worse by a change in your physical activity?
Is your doctor currently prescribing drugs (for example, water pills) for your blood pressure or heart condition?
Do you know of any other reason why you should not do physical activity?
As always, please reference my disclaimer regarding medical advice.
First, record your baseline VO2 max using one of the measurement tools listed above.
For a period of six to eight weeks, plan to devote three days per week to interval training, which may consist of walking, running, cycling, or rowing. Following the completion of your training block, calculate your VO2 max again.
Here’s to your health!