





The hottest new trend in personalized health might be the continuous glucose monitor (CGM). Typically inserted along the tricep or abdomen, this small device provides real-time data about blood sugar levels, usually accessible on a smartphone app.
CGMs are an increasingly vital tool for patients who do not produce insulin (in type 1 diabetes and severe type 2 diabetes) and those who are insulin resistant (other forms of type 2 diabetes). CGM data help to determine the amount of insulin injected after a meal to avoid high blood glucose (hyperglycemia), identify triggers for hyperglycemia, and monitor for episodes of low blood glucose (hypoglycemia).
Certain start-ups now advertise CGMs to healthy people without diabetes. Their pitch is speciously intuitive— increased variability and “spikes” in blood sugar are harmful to health and contribute to metabolic dysfunction. Using CGM to track how food, sleep, exercise, and stress affect blood glucose can minimize spikes and variability, optimizing our health.
This line of reasoning perpetuates a fantastic grift, exploiting well-meaning intentions to improve health through lifestyle change. Unfortunately, claims made by CGM start-ups rely on weak evidence, oversimplify insulin resistance, and might actually be harmful. Guarding against metabolic disease is imperative, but tracking minute changes in our blood chemistry should likely not be among our concerns. At worst, such focus may lead one down the garden path and promote metabolic dysfunction.
This piece examines the physiology of blood glucose, the major contributors to insulin resistance, the limited utility of CGM in healthy patients, and more reliable assessments of metabolic health.
Just a Spoonful of Sugar
Blood glucose is tightly regulated by a near-constant interplay of hormones and feedback mechanisms. After fasting for about eight hours, blood glucose in healthy individuals tends to be below 99 mg/dL, although some organizations define the upper limit of normal at 110 mg/dL. Conventionally, a fasting blood glucose between 100 to 125 mg/dL is diagnostic for prediabetes (at heightened risk for developing type 2 diabetes) whereas a level above 126 mg/dL on two or more separate tests helps to diagnose type 2 diabetes, which is defined by insulin resistance.
Insulin is the only hormone in the human body that lowers blood sugar. Released from beta cells in the pancreas, insulin signals the liver, skeletal muscle, heart muscle, and adipose tissue to absorb glucose through special membrane channels. All other organs and cell types take in glucose independently of insulin. Glucose is then used to generate energy in the form of adenosine triphosphate, or ATP.
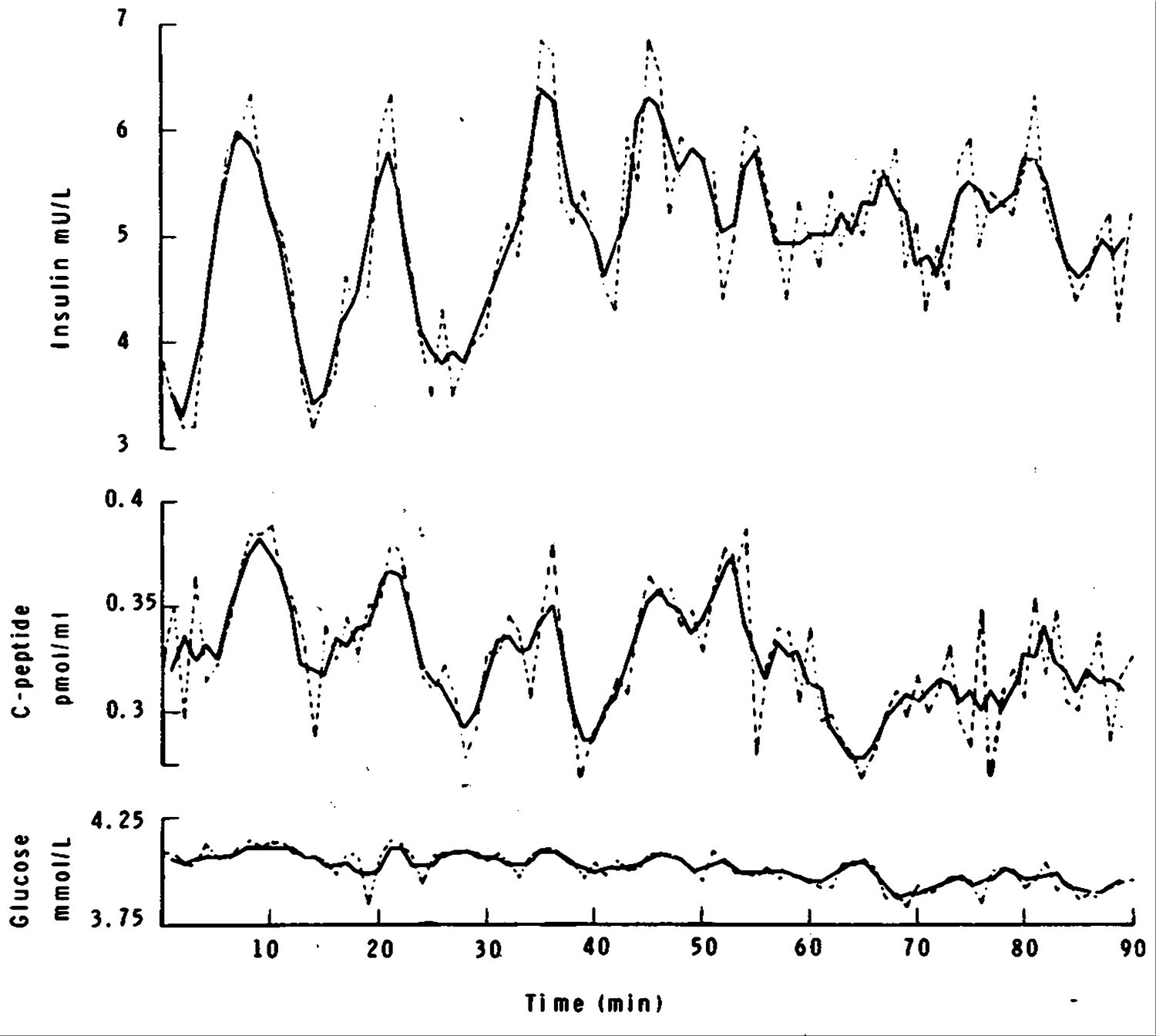
Insulin is normally secreted in a pulsatile manner with distinct bursts rather than a continuous, steady release. In healthy individuals, low levels of insulin are secreted every four to eight minutes when blood glucose levels are between 80 to 120 mg/dL, independent of a meal.
Within ten minutes of consuming a meal with carbohydrates, blood glucose begins to rise. After one to two hours, blood glucose usually reaches its peak in healthy individuals at about 140 mg/dL or lower. After this brief pulse, levels gradually decrease as glucose is taken up from circulation in response to insulin.

Besides fasting values, blood glucose levels after a meal (called “postprandial”) can also be used diagnostically. In an oral glucose tolerance test (OGTT), a patient consumes 75 grams of glucose after fasting for at least eight hours. Their blood glucose is measured two hours later: a healthy result is 140 mg/dL or lower, whereas prediabetes is marked by levels between 141 to 199 mg/dL. Blood glucose of 200 mg/dL or above is diagnostic of diabetes.
As diet, sleep, stress, and exercise contribute considerable variability in daily blood glucose levels, measuring average values over time tends to provide deeper insight into metabolic health.
Hemoglobin A1c (HbA1c) is currently held as the gold standard for diagnosing prediabetes and diabetes. HbA1c measures the degree to which hemoglobin, a protein in red blood cells (RBCs), is glycated (glucose becomes attached), indicating average blood glucose levels over the last 2-3 months. An A1c below 5.7% is defined as “normal.” A level between 5.7% to 6.4% denotes prediabetes. 6.5% and above is diagnostic for type 2 diabetes.
Things Fall Apart
In states of insulin resistance, physiologic levels of insulin are unable to produce a normal response in target organs and tissues. As a result, these cells absorb less glucose from circulation, leading to greater variability in blood glucose and higher average levels.
The mechanistic and morphologic alterations that underlie insulin resistance are fundamentally similar to other states in which the body becomes less sensitive to a molecular signal:
Fewer receptors for the signaling molecule are present
HOW: fewer receptors are produced; receptors are not transported to the proper location; accelerated degradation of receptors
Receptors have a reduced ability to bind the signaling molecule (affinity)
HOW: DNA mutations; epigenetic changes; other molecules competitively or non-competitively bind to the same receptor
The signaling pathways initiated by the receptor after binding the signaling molecule are disrupted (efficacy)
HOW: DNA mutations; epigenetic changes; other molecules (including antibodies) competitively or non-competitively bind to the same receptor; other molecules bind to different receptors, which modulate neighboring signaling pathways
Antibodies sequester the molecule, preventing it from reaching its receptor
This mechanism is fairly rare in insulin resistance but has been observed, mainly induced by exogenous insulin administration.
Production or function of transport proteins that carry the signaling molecule in the blood or cell is disrupted
This mechanism notably does not apply in insulin resistance-— insulin travels in the blood without a transport protein.
Some signaling molecules, such as thyroid hormones, are transported in blood by a carrier molecule.
These modulations may occur simultaneously and exist transiently or chronically, producing variable effects in sensitivity to a molecular signal.
Numerous conditions prompt changes that reduce insulin sensitivity, including puberty, pregnancy, older age, organ damage, certain cancers, certain medications, starvation, and obesity, mainly through visceral fat accumulation.
Additional processes that contribute to insulin resistance include acute or critical illness (such as a traumatic injury or an infection), mitochondrial dysfunction, low levels of physical activity, and hyperinsulinemia (chronically elevated insulin levels).
While reduced sensitivity to insulin can be a natural, transient phenomenon, avoiding chronic insulin resistance is paramount. Diabetes is among the most common causes of mortality and wreaks havoc on the kidneys, eyes, heart, blood vessels, immune system, and nerves. Given this diverse impact, some are bold enough to state they would rather have HIV than diabetes. Effective anti-retroviral treatments for HIV nearly extinguish all harms from the condition, enabling a normal life expectancy. The same sadly cannot be said for diabetes.
A Shill Game
Given these ruinous consequences, preventing metabolic disease is top of mind for many. Some gravitate to trusted figures on social media to learn how to improve metabolic health. Unfortunately, the answers found there are sometimes little more than a veiled sales pitch.
Certain health influencers (examples here, here, and here) spread the claim that blood sugar “spikes” are ipso facto suboptimal for health, usually without explanation or scholarly attribution. If one feels tired, sluggish, run-down, or burn-out, you should apparently blame your blood sugar. Purchasing a CGM (using the influencer’s referral link, of course) is presented as the best way to avoid these spikes and improve metabolism.
When non-diabetics use CGM, they likely only observe their bodies’ somewhat boring physiology in action. Certain meals will elevate blood glucose. Insulin will be secreted by the pancreas. The liver, heart, muscle, and adipose tissue will respond to this hormonal signal, and blood glucose will gradually decrease to baseline levels.
Notably, some healthy individuals could see a pulse in postprandial blood glucose above 140 mg/dL, the putative threshold for prediabetes, or even 200 md/dL, the cut-off for diabetes. These data points might be alarming to observe, but limited data suggest that non-diabetics spend 6 to 12 to 30 to 45 minutes each day with blood glucose above 140 mg/dL. There is no evidence to suggest these brief periods of increased blood glucose are as deleterious as chronic hyperglycemia.
Even if CGM data do reveal prolonged excursions in postprandial blood glucose, these devices are not validated to diagnose or screen for diabetes. Any potential insights rendered from these data will necessitate further clinical testing, requiring further expense for the patient (and, most likely, health insurance companies).
Beyond blood sugar “spikes,” health influences also attack glycemic variability (GV), the degree of fluctuation in blood glucose throughout the day.
Some influencers and CGM start-ups reference a compelling argument that increased GV could signify a prodrome of prediabetes not currently captured by conventional screening protocols. A CGM could therefore reveal that an individual with “normal” HbA1c, fasting blood glucose, or OGTT may nonetheless have considerable GV, increasing their risk for diabetes. Armed with this enhanced risk prediction, patients can implement lifestyle changes sooner to forestall metabolic disease.
Admittedly, this scenario would be an excellent use case for CGMs in non-diabetics, but there are currently no longitudinal clinical data to support this claim. It is not currently known if GV in healthy individuals influences the incidence of insulin resistance, type 2 diabetes, or other hard clinical endpoints. These are undoubtedly vital research questions; we just do not possess the epistemic clarity that start-ups suggest in their pitches.
In the meantime, HbA1c remains the best clinical tool available to monitor the risk of developing diabetes. A large body of work also shows GV tends to have a positive association with HbA1c. Even if GV eventually proves to have robust predictive value, tracking HbA1c instead of using a CGM is unlikely to be detrimental in the present day.
The Cure is Worse than Causes the Disease
Even in the absence of firm evidence, some may choose to take an aggressive approach in preventing metabolic disease and utilize a CGM. Besides the expense of a few hundred dollars per month, is there any harm in this approach?
As we have seen, CGM data provide a great deal of noise but not necessarily a clear signal, given that the pathologic significance of brief “spikes” in blood sugar and glycemic variation in healthy individuals is not firmly established. Again, these devices cannot actually screen for diabetes either.
Beyond financial loss, the actual risk in using CGM comes with the coaching provided by most start-ups in smartphone applications. Users quickly learn about the “triggers” that temporally contribute to blood sugar “spikes,” including sleep deprivation, psychological stress, illness, and certain food items. Users are advised to avoid these triggers to promote glycemic stability and improve their metabolic health.
As most excursions in blood glucose occur with eating, CGM coaching largely focuses on the role of dietary choices— particular foods will lead to more “spikes'' and should therefore be avoided. Because there is wide variation in how individuals respond to different food items, CGM data allow users to uniquely tailor their diets to optimize metabolic health. That is the pitch, at least.
Here is the risk: meals that are proportionally higher in protein and fat than carbohydrates will inevitably reduce glycemic variability on a CGM. These dietary choices may include more animal protein, more saturated fat, and less fiber, which each have the potential to worsen underlying insulin resistance despite the spurious improvement in CGM data.
The dietary patterns promoted by CGM coaching may also more consistently place individuals in an energy surplus (i.e., caloric intake exceeds energy expenditure) given the caloric density of fat. Consistent overfeeding runs the risk of increasing visceral fat, among the most significant contributors to insulin resistance.
Yet worse, certain influencers and start-ups vilify foods that may actually help to improve insulin sensitivity, such as those high in fiber. Oatmeal, for instance, is deemed a “sneaky spiker” of blood sugar. The rating system in some CGM apps may even report a standard burger and fries is a better option than oats for certain individuals.
CGM start-ups further encourage these suboptimal behavioral changes with unsound guidance for blood glucose targets. Levels, for instance, recommends that “optimal” postprandial blood sugar should never exceed 110 mg/dL. This guideline is not based on rigorous clinical research but rather an observational study funded by a CGM manufacturer over two days. No meaningful clinical outcomes were assessed. Do we know if this exacting glycemic control reduces the incidence of type 2 diabetes or atherosclerotic disease over, say, two years or five years? No, we do not.
Some may accept the premise that CGM coaching entrains behaviors that may harm metabolic health by reducing insulin sensitivity but find it meaningless. What does it matter if a CGM user becomes more insulin resistant if they plan to maintain strict glycemic control anyway?
Recall that insulin is practically always secreted at a basal rate. The pancreas never rests. If an individual continually loses insulin sensitivity, their fasting blood glucose will increasingly escalate towards pathologic levels no matter their diligence in avoiding “triggers.” To limit the sequelae of chronic hyperglycemia, this person ends up using CGM not unlike an individual with prediabetes or type 2 diabetes, the very conditions they were hoping to avert.
In this respect, the cure is the same as the disease.
The Path from Here
Absent robust data showing that glycemic variation and brief periods of hyperglycemia influence clinical endpoints in healthy people, non-diabetics can safely ignore suggestions that CGMs are a vital tool in optimizing metabolic health.
Regularly monitoring HbA1c remains our best strategy to understand risk for developing type 2 diabetes. Instead of striving to avoid blood sugar “spikes,” focus can shift towards cultivating a healthy lifestyle that limits visceral fat accumulation through frequent physical activity, refraining from habitual energy surplus, smoking cessation, and moderating alcohol intake.

Further Reading
The growing use of continuous glucose monitors in people without diabetes: an evidence-free zone, Nicola Guess RD, MPH, PhD
Is Glucose the New Gluten? Inside the Blood-Sugar Health Craze, Wall Street Journal
Personalized Nutrition Programs Are Making People Feel Weird About Food, WIRED
Always extremely informative, these hard looks at the factors adding to the health ‘plague’ affecting so many in this country (and beyond?).
This series may act to expand the understanding by all of those challenged by this overall diverse malady of present day society/culture