

How Low Should You Go?
Moving the Goal Posts for Cholesterol

Odds are you would prefer not to die from a heart attack or stroke. You probably do not want diabetes, dementia, or kidney disease listed as contributors on your death certificate either.
My piece This is How You Will Die examines a common denominator among these disease processes: atherosclerosis, the presence of cholesterol plaques in the walls of arteries.

It is far from hyperbole to state that atherosclerosis is the most meaningful source of morbidity and mortality in the world. Worse still, it is almost entirely preventable.
Atherosclerosis is currently understood to be initiated by damage to the arterial wall largely from high blood pressure, metabolic dysfunction, and smoking. This damage activates immune pathways that cause inflammation and enable infiltration of cholesterol and their carriers, lipoproteins, into the vessel wall leading to plaque formation. Low-density lipoproteins, LDL, are the most common; cholesterol carried by LDL is called LDL-C.
Without healthy blood pressure, robust metabolic health, and smoking cessation, lowering cholesterol alone will not be as potent in decreasing atherosclerosis. Nonetheless, reducing LDL-C is one of the most impactful actions we can take for the length and quality of our lives.
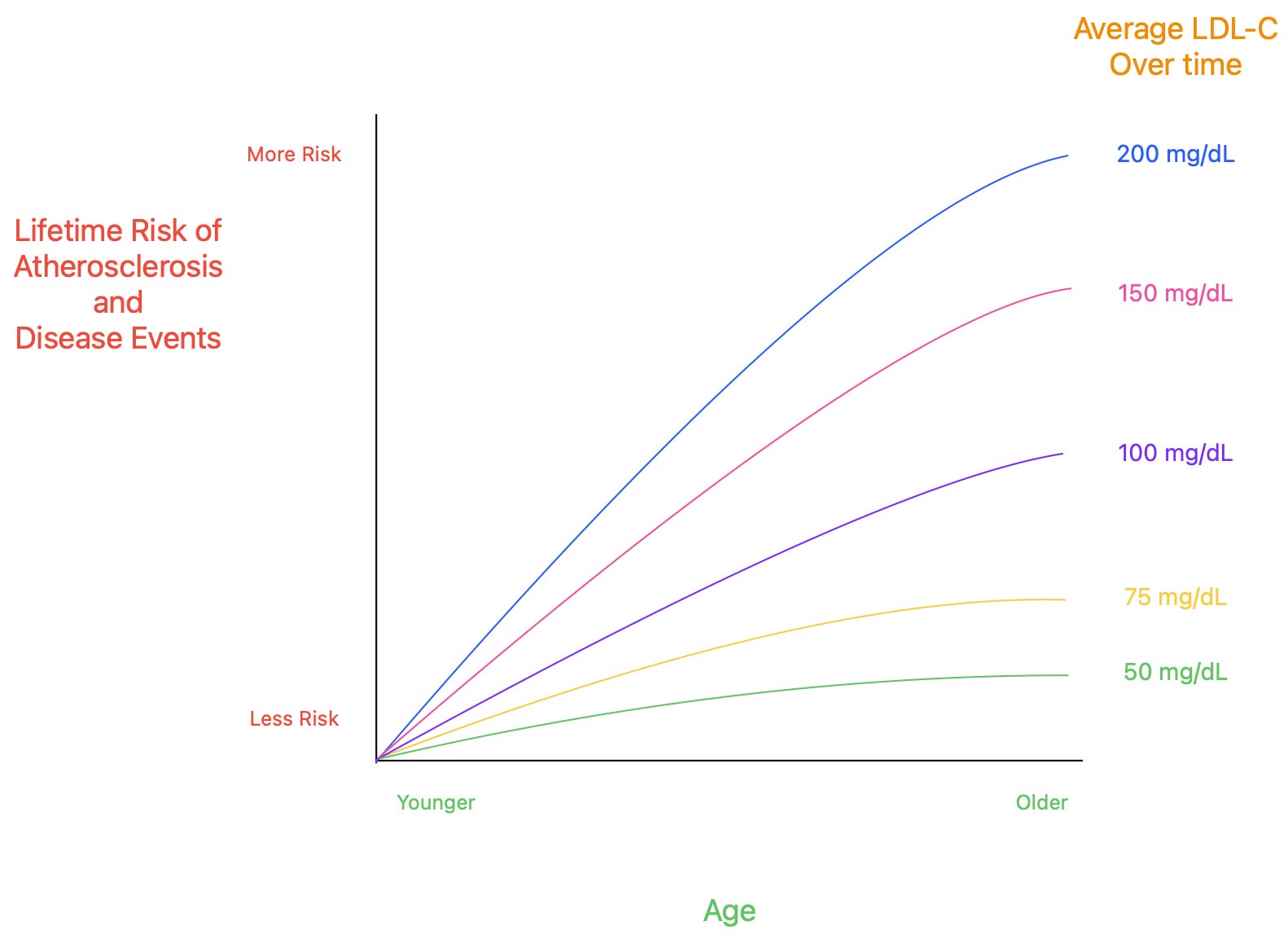
Broadly, the lower the better, the earlier the better, the sooner the better. (Inspired by Steinberg & Grundy (2012).)
Our starting goal should be an LDL-C level below 70 mg/dL, although maintaining the lowest possible level (lower than 30 mg/dL) starting as early in life as possible is ideal. A lipid panel should be monitored at least once every three years; every year is preferable if implementing changes. These recommendations are based on insights from emerging research:
There is a linear dose-response relationship between LDL-C and atherosclerosis and its attendant disease events, such as heart attacks and strokes. Lower LDL-C = less atherosclerosis and fewer events. This linear relationship holds in multiple studies, ranging from LDL-C of 200 mg/dL to below 10 mg/dL.
Exposure to LDL-C over the lifespan meaningfully influences progression of atherosclerosis and atherosclerotic disease events.
Lower LDL-C maintained starting early in life confers lower lifetime risk of atherosclerotic disease
If conditions that damage the arterial wall are not well managed, decreasing LDL-C might be insufficient to reduce atherosclerosis.
Plaque progression and atherosclerotic disease events are still observed when LDL-C is below 10 to 20 mg/dL, almost always in the setting of multiple other risk factors for atherosclerosis.
Taken together, these insights underscore the goal of maintaining very low levels of LDL-C starting early in life to minimize the development of any plaques, given that they may be nearly impossible to reverse. This goal should be pursued in tandem with managing high blood pressure, high blood sugar, and smoking.
The Current Paradigm
Primary prevention refers to actions taken to prevent disease before it has started (e.g., a vaccine to prevent Hepatitis B)
In this context, our goal is to prevent the formation of new atherosclerotic plaques.
Secondary prevention refers to actions taken to identify early-stage disease and prevent further progression (e.g., a colonoscopy to detect colon cancer)
In this context, our goals are:
Stabilize current plaques and stop them from growing further;
Decrease the size of current plaques.
A statin is a safe, commonly used medication that inhibits cholesterol synthesis in the liver. Lower cholesterol content in the liver up-regulates LDL receptors, which pull LDL out of the blood.
A statin might be effective on its own or paired with additional medications.
In the UK, certain formulations of statins are available over the counter without a prescription.
The primary prevention paradigm for atherosclerotic cardiovascular disease (ASCVD) risk typically takes into account a patient’s age, family history of heart disease, and diabetes in determining a target for LDL-C.
An LDL-C level below 100 mg/dL is generally considered “healthy” by most clinical guidelines.
At levels between 100 to 190 mg/dL, clinicians may recommend starting a statin for patients at increased ASCVD risk.
At levels above 190 mg/dL, clinicians will most likely initiate a statin independent of calculated ASCVD risk and recommend additional testing for genetic conditions that predispose to high cholesterol levels.
For those aged 40-75 with diabetes, a statin is recommended independent of LDL-C levels, given enhanced risk for ASCVD.
The secondary prevention paradigm for ASCVD risk is much more straightforward:
LDL-C target is 70 mg/dL or lower, achieved through medical therapy.
The 2019 European Society of Cardiology recommend an LDL-C target less than 55 mg/dL.
Reversing Atherosclerosis
Atherosclerotic plaques can be identified in several ways:
Imaging, such as an invasive study of arteries or a less-invasive cardiac CT scan or cardiac MRI
Clinical inference from current conditions like angina (chest pain during exertion) or claudication (calf pain during exertion)
Previous atherosclerotic events like a heart attack, ischemic stroke, or limb ischemia.
Plaque reduction appears to first occur when LDL-C levels reach somewhere between 65 to 70 mg/dL. This is an average and not true for every individual.
Even at levels below 70 mg/dL, plaque volume continues to decrease for most individuals in a linear fashion as shown in the GLAGOV trial, the HUYGENS trial, and a meta-analysis of statin trials. Thus far, there is no established limit at which decreases in LDL-C no longer correspond to plaque regression. Even at LDL-C levels as low as 20 mg/dL (GLAGOV trial), plaque regression continues to be observed.
{kind=link}
Of course, we only care about plaque reduction because it reduces mortality from atherosclerosis. Each 1% reduction in atherosclerotic plaque volume corresponds to a 20% reduction in the odds of incurring death, heart attack, and stroke.
Indeed, this linear dose-effect relationship holds for atherosclerotic disease events, which decrease monotonically with LDL-C levels as low as 10 mg/dL (FOURIER trial) to 20 mg/dL (meta-analysis of statin trials).

At the same time, this work carries rather chilling observations. In the GLAGOV trial, about one-third of subjects actually had plaque progression with LDL-C levels in the 30s over a median follow-up of 1.5 years. Similar observations are found in the appendix for a secondary analysis of the FOURIER trial. 7.3% of patients who achieved LDL-C levels below 10 mg/dL still experienced a cardiovascular death, heart attack, stroke, hospitalization for unstable angina, or placement of a coronary stent over a median follow-up of 2.2 years.
A post-hoc analysis of the GLAGOV trial found that subjects with plaque progression despite very low LDL-C had higher baseline HbA1c, higher systolic blood pressure, and lower plaque volume. The more baseline risk factors for atherosclerosis present, the higher incidence of plaque progression.
In other words, forgoing management of conditions that harm the arterial wall will make atherosclerotic reversal less likely to occur at very low LDL-C, and risk for atherosclerotic disease will remain unnecessarily high.
Preventing Plaques
If we intend to minimize our lifetime risk of atherosclerosis, we must act to prevent the formation of plaques from the outset.
This goal requires action to curtail arterial wall damage, the inciting event for atherosclerosis. Beyond conventional risk factors, there is emerging evidence that sleep deprivation, air pollution, and the microbiome may separately promote inflammatory pathways that influence atherogenesis, suggesting we likely cannot avoid all sources of damage to the arterial wall despite behavioral change.
Ineluctable endothelial dysfunction therefore requires that LDL-C is reduced to the lowest possible level to prevent the development of clinically significant plaques. As the above data suggest, there is no lower limit at which reducing LDL-C ceases to decrease risk from atherosclerosis. Thus, the lower the better.
Copious evidence demonstrates this low LDL-C should be maintained starting in childhood to minimize atherosclerosis over the lifespan. Nearly half of all infants under one year of age sampled in autopsy studies already show evidence of fatty streaks, the precursor lesion to atherosclerotic plaques. By age ten, all children sampled have fatty streaks in segments of their arteries.
Fatty streaks on their own do not cause disease but instead load the metaphorical gun for atherosclerosis. Persistent arterial wall damage and elevated lipids will then pull the trigger.
Ference et al. (2018) elegantly advance the concept that development of atherosclerosis is meaningfully influenced by cumulative LDL exposure over time. Namely, they propose there is a threshold of cumulative exposure after which ASCVD risk increases significantly.
Let’s say a 40-year-old patient obtains a lipid panel for the first time in their life, and their LDL-C is measured at 200 mg/dL. Given a lack of historical data, it is impossible to know whether their LDL-C was consistently elevated for decades or if this level signifies a relatively recent rise.
According to the exposure argument, there is higher risk conferred from consistently elevated LDL-C levels compared to an elevated level reached only recently. This conclusion may seem intuitive to some readers— because it is— but cumulative exposure has not been integrated into clinical guidelines. The current paradigm is guided only by contemporary (i.e., one time) LDL-C values, which clinicians may only measure sparsely early in life.
Work by Zhang et al. (2021) finds that lower cumulative exposure to LDL-C corresponds to lower lifetime incidence of ASCVD, independent of the LDL-C level measured in middle age.
Given this result, they conclude (emphasis mine):
“… incorporating serial LDL-C measures and cumulative LDL-C burden into clinical practice may further refine CVD [cardiovascular disease] risk assessment and help inform strategies for primary prevention of CHD [coronary heart disease]. Moreover, given that the risk of developing atherosclerotic plaques and CHD events is associated with the cumulative exposure to LDL-C, it is plausible that achieving optimal lipid levels early in life and maintaining those optimal levels throughout adulthood may prevent incident CHD events better than the current paradigm of deferring lowering LDL-C levels to later in life when atherosclerosis is likely already advanced.”
Natural experiments examining individuals with genetic mutations that lower LDL-C starting at birth confirm that lower levels over the lifespan confer significantly decreased risk of coronary heart disease.
This argument is further bolstered by research suggesting exposure to LDL-C earlier in life has a larger impact on ASCVD risk compared to commensurate LDL-C exposure later in life. Domanski et al. (2020) find (emphasis again mine):
“Individuals with higher LDL-C early (18 to 30 years of age) followed by lower LDL-C between ages 30 and 40 years had a greater risk of an incident CVD event after age 40 years than individuals with lower LDL-C between ages 18 and 30 years but then higher LDL-C when both groups had achieved the same cumulative area at age 40 years. Taken altogether, these data show that the risk of CVD depended on both the cumulative exposure to LDL-C and also, importantly, the time course of area accumulation.
Individuals with the same cumulative LDL-C exposure at age 40 years … but with a greater fraction of that exposure occurring earlier in life had a greater risk of incident CVD events subsequent to age 40 years.”
It is never too soon to begin addressing atherosclerosis. The earlier the better. The sooner the better
In sum, minimizing atherosclerosis necessitates that one achieves low levels of LDL-C as early in life as possible and consistently maintain low levels. At the same time, it remains vital to manage high blood pressure, high blood sugar, and smoking to prevent arterial wall damage.
LDL-C should be measured serially (ideally annually or at least once every three years). A good initial target for LDL-C is below 70 mg/dL, though ideally one achieves as low a level as possible through lifestyle modification and medical therapy starting as easy in life as possible. Both approaches are discussed more exhaustively in This is How You Will Die.
Additional Reading
Impact of Lipids on Cardiovascular Health, Ference et al. 2018
There is urgent need to treat atherosclerotic cardiovascular disease risk earlier, more intensively, and with greater precision, Makover et al. 2022